
Did you know that during the 1930s–1950s, tobacco companies paid actors dressed as doctors and even worked with real physicians to promote cigarettes?
Some ads said: “More doctors smoke Camels than any other cigarette.”
This was part of a strategy called “white coat marketing1,” where the image of doctors was used to create brand trust.
At the same time, ads marketed cigarettes to pregnant women as a way to manage weight gain and calm nerves. Some even implied smoking made you a better mother by helping you stay slim and stress-free.
In the 1930s and early 1940s, German doctors were the first to link smoking to lung cancer. But because that research came out of Nazi Germany2, where it was tied to a disturbing obsession with control and national “purity,” the rest of the world ignored it after WWII, and later credit for the discovery was given to British and American scientists in the 1950s.
Tobacco companies quickly jumped on the confusion. They turned smoking into something “healthy,” glamorous, and patriotic, hiding the harm behind marketing, money, and freedom.
This might sound unrelated, but today, something similar is happening with food, especially carbohydrates. Instead of cigarettes, fiber, fruit, and real food are being labeled as unhealthy and “bad.”
Carb Fear Isn’t New
Diet trends, nutrition headlines, and misinterpreted advice have all contributed to carb fear.
As much as people like to blame social media’s popularity for everything, it didn’t create the problem; it just gave people (influencers) a way to repeat what they heard and share it. But just like old-fashioned marketing campaigns, some are in it for the wrong reasons.
So, now, even when we try to set the record straight, the comment sections show how deep the confusion still runs. People have been led to believe that the word “carb” automatically means weight gain and high blood sugar.
How Carb Fear Took Over
Carbs didn’t become a problem overnight. It had been building up for decades, but it hit hard in the late 1990s and early 2000s, especially with the rise of the celebrity-endorsed Atkins3 Diet. That’s when “cutting carbs” became trendy.
1970s–1980s: “Fat is the enemy”
Dr. Atkins’ Diet Revolution was published in 1972, but it wasn’t mainstream at that time because this was the era of low-fat, high-carb eating backed by:
- The 1977 U.S. Dietary Guidelines
- Well-known physiologists and researchers like Ancel Keys, who pushed the idea that dietary fat, especially saturated fat, was the leading cause of heart disease.4
The science wasn’t wrong, but public health campaigns took the “fat causes heart disease” idea and ran with it.
Instead of teaching people to eat better fats and more whole foods, the message became: cut all fat, and eat anything labeled “low-fat.”
Corporate America heard this loud and clear, so they started producing and marketing sugary low-fat yogurts, snack bars, and pasta-heavy meals, even though that was not the advice given.
What the 1977 Guidelines Recommended
The 1977 Dietary Goals for the United States5 did not trash all fats or promote unlimited caloric or carbohydrate intake, but they did tell people to:
- Reduce their total fat intake from about 40% to 30% of daily calories.
- Limit their saturated fat intake to 10% of daily calories.
- Increase their complex carbohydrates and naturally occurring sugars (like those in fruits and vegetables) from about 28% to 48% of daily calories.
- Reduce their refined and processed sugars to about 10% of daily calories.
These recommendations tried to shift the standard American diet6 towards more whole grains, fruits, and vegetables, and away from saturated fats and added sugars.
Even then, they weren’t saying to cut everything and only eat perfect whole foods.
The message was more like: find some balance, eat less of the boxed stuff and more of the real stuff.
Where Things Went Off Track
The food industry and public interpretation misunderstood and misused the recommendations:
- To make low-fat products taste better, manufacturers packed them with sugar and refined carbs.
- “Low-fat” labels made processed food look healthy.
- People ate more, not better (think fat-free cookies and sugary cereals).
1990s: Carbs Become the New Enemy
Even though everyone was obsessed with low-fat everything, obesity rates didn’t slow down. In fact, this shift may have played a role in rising obesity rates.7 Here’s what the data shows:
- In the early 1970s, obesity in U.S. adults was around 14–15%.
- By the mid-1990s, it was closer to 23–25%.
- By the early 2000s, it was over 30%, and it’s continued to rise since.
So, naturally, we had to find something else to blame.
“Wait, so we cut fat, but we’re still gaining weight. It’s got to be the carbs!”
This is when Atkins resurfaced, keto caught on, and soon “low-carb” replaced “low-fat” and got slapped on every product.
All breads, fruit, and oatmeal suddenly became nutritionally equivalent to candy bars and donuts.
Was the Science Wrong?
Not really.
Early science showed that reducing saturated fat could help lower cholesterol. But we didn’t fully understand what happens when people replace fat with processed sugar.
Later research revealed that diets high in refined carbs raise the risk of metabolic disorders, like heart disease, prediabetes, and type 2 diabetes.
It wasn’t the carbs but the kind of carbs and how we responded to the message.
Why Are Carbs Still Misunderstood?
We can certainly blame diet culture, but a lot of it does come down to a lack of solid nutrition education:
- Most people don’t know the difference between carbs from a sweet potato and a Pop-Tart.
- Or that carbs support energy, thyroid function, hormone balance, and workout recovery.
- Or that fiber is an important type of carb.
Facts are facts. Carbs are not the enemy, but too many ultra-processed, low-nutrient (simple) carbs can lead to overeating and weight gain, mainly because you’re taking in more energy than you’re using.
What Is a Carb?
Simple Carbs Are Short-Chain Sugars
Found naturally in fruit and milk, but also heavily refined in junk foods like:
- Soda
- Candy
- Pastries
- White bread
- Most packaged snack foods
The body digests them quickly, which can cause blood sugar spikes and less satiety, especially when eaten without protein or fiber.
That said, a small amount of simple carbs can be helpful before a workout if you need quick energy.
They help after a workout, too, especially when combined with protein to refuel your muscles.
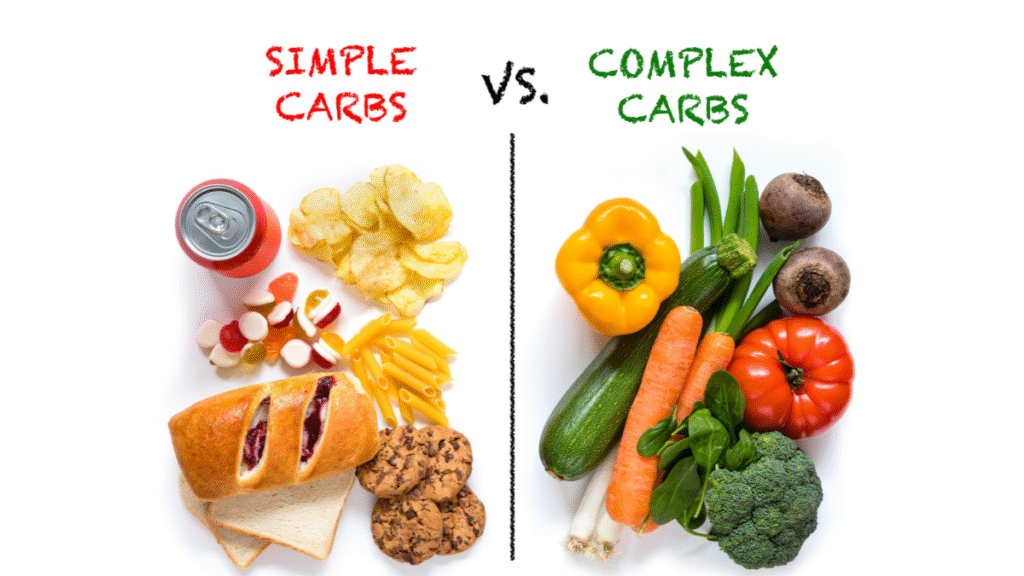
Complex Carbs Are Longer Chains and Contain More Nutrients
They digest more slowly and provide fiber, vitamins, and minerals.
Fiber is a type of complex carb that your body doesn’t fully digest, so not all the carbs in high-fiber foods get converted into blood sugar.
Plus, it supports digestion, helps you feel fuller longer, and plays a key role in gut health (it feeds your gut bacteria, think prebiotic).
Found in:
- Vegetables
- Whole grains (like oats, quinoa, brown rice)
- Legumes
- Beans
- Root veggies (like sweet potatoes)
How Low-Carb Messaging Messes with GLP-1 Progress
For women on GLP-1s, fear of carbs shows up differently. It’s not just old diet culture stuff, because some GLP-1 users are already dealing with:
- Exhaustion or low energy throughout the day
- Reduced motivation to move or exercise
- Rapid weight loss (sometimes way faster than your body can keep up with)
- Constipation, nausea, and GI slowdown from slower digestion and lower food volume
Cutting carbs on top of that removes your body’s main energy source and often makes digestion even worse. GLP-1 meds already slow down digestion, so fiber needs to be added gently. But the right kind, in the right amount, can actually help reduce nausea, support regularity, and stabilize energy.
And when you cut carbs too low for too long, you’re also looking at:
- Lower workout performance: Without that quick-access energy, it’s harder to strength train or even do walking-based workouts.
- Less support for muscle retention: When calories are already low, missing carbs puts your lean tissue at even more risk.
That’s how strength, stamina, and metabolism start to decline, even if you’re still on the meds.
High-fiber carbs like fruits, veggies, oats, and beans can help:
- Replenish energy stores (glycogen)
- Support muscle retention when calories are low
- Improve digestion and help regulate constipation if introduced slowly, and you’re drinking enough water.
So, while things like Metamucil, psyllium husk, or other fiber supplements can help, real-food sources of fiber from carbohydrates can do the same job with added nutrients.
Low-Carb Messaging Reinforces Disordered Food Beliefs
A lot of women taking GLP-1 meds have already spent years (if not decades):
- Chronic dieting
- Feeling guilty about food
- Black-and-white thinking (“all carbs are bad, no exceptions”)
This keeps them stuck in cycles of:
- Removing entire food groups, not just because they’re not as hungry as before, but because they’ve been told carbs will “cancel out” their progress
- Eating the protein, pushing away the fruit or grains, because they’re afraid even healthy carbs will cause weight gain
- Avoiding higher-fiber carbs like beans, oats, or sweet potatoes, even when they’re constipated, because they don’t realize those carbs will actually help
- Panicking at the idea of a “carb target” or macro goal, because it seems way too much
The 1977 guidelines meant well; they were trying to improve public health by cutting saturated fat and encouraging more complex carbs. But the message got twisted. Instead of promoting balance, it turned into another marketing free-for-all.
It’s not just what we say about nutrition, it’s how we say it. If the message isn’t clear or realistic, people can’t apply it in real life.
And lasting change doesn’t come from adding more food rules. It comes from rebuilding trust with yourself around food.
Final Thought
Dr. Atkins died at 72 after slipping on ice and hitting his head.
Some reports said he had heart issues before he passed away, but he and his wife pushed back on that, saying his labs looked good and the cardiac episode he had previously was from a virus, not his diet. There’s still debate, and no one really knows the full story.
But here’s where my trainer brain kicks in: When you eat super low-carb for years, your energy and muscle can take a hit. And if you’re not fueling right or moving enough, your body just doesn’t bounce back the same way, especially as you get older. I’m not saying that’s why he fell. But I’ve always wondered if not eating enough for so long left him feeling weak, off balance, or just not as strong as he once was.
We’ll never know for sure, but it’s a reminder that being healthy isn’t just about what you cut out; it’s about what you build up. Energy, strength, stability… those things matter more than any headline diet rule.
Carbs aren’t the enemy, but the hard part is unlearning all the crap we’ve been told about them. Weight gain isn’t just about eating carbs; it’s about overall intake. Let’s stop repeating history and being afraid of food that fuels us.
Resources
- Pharmacy Times, Marketing Arrangements Spark Concerns for Specialty Pharmacies, https://www.pharmacytimes.com/view/marketing-arrangements-spark-concerns-for-specialty-pharmacies ↩︎
- Wikipedia, Anti-tobacco movement in Nazi Germany, https://simple.wikipedia.org/wiki/Anti-tobacco_movement_in_Nazi_Germany ↩︎
- NIH NCBI, Lenzer J. Robert Coleman Atkins. BMJ. 2003 May 17;326(7398):1090. PMCID: PMC1126011., https://pmc.ncbi.nlm.nih.gov/articles/PMC1126011/#:~:text=Robert%20Coleman%20Atkins%2C%20founder%20and,on%20a%20New%20York%20sidewalk. ↩︎
- NIH NCBI, The Lipid–Heart Hypothesis and the Keys Equation Defined the Dietary Guidelines but Ignored the Impact of Trans-Fat and High Linoleic Acid Consumption, Newport MT, Dayrit FM. The Lipid-Heart Hypothesis and the Keys Equation Defined the Dietary Guidelines but Ignored the Impact of Trans-Fat and High Linoleic Acid Consumption. Nutrients. 2024 May 11;16(10):1447. doi: 10.3390/nu16101447. PMID: 38794685; PMCID: PMC11123895., https://pmc.ncbi.nlm.nih.gov/articles/PMC11123895/#:~:text=Abstract,and%20the%20lipid%E2%80%93heart%20hypothesis. ↩︎
- Dietary Guidelines of America, History of the Dietary Guidelines, https://www.dietaryguidelines.gov/about-dietary-guidelines/history-dietary-guidelines#:~:text=To%20avoid%20overweight%2C%20consume%20only,about%205%20grams%20a%20day. ↩︎
- NIH, NCBI, Overview of Health and Diet in America, Institute of Medicine (US) Committee on Examination of Front-of-Package Nutrition Rating Systems and Symbols; Wartella EA, Lichtenstein AH, Boon CS, editors. Front-of-Package Nutrition Rating Systems and Symbols: Phase I Report. Washington (DC): National Academies Press (US); 2010. 4, Overview of Health and Diet in America. Available from: https://www.ncbi.nlm.nih.gov/books/NBK209844/, https://www.ncbi.nlm.nih.gov/books/NBK209844/ ↩︎
- NIH, Explaining adult obesity, severe obesity, and BMI: Five decades of change, Kranjac AW, Kranjac D. Explaining adult obesity, severe obesity, and BMI: Five decades of change. Heliyon. 2023 May 19;9(5):e16210. doi: 10.1016/j.heliyon.2023.e16210. PMID: 37251838; PMCID: PMC10213181., https://pmc.ncbi.nlm.nih.gov/articles/PMC10213181/#:~:text=Average%20population%20BMI%20and%20obesity,%25%20(25.7%20to%2029.8). ↩︎
Photo Credits
Dietary fiber food shot from above by fcafotodigital from Getty Images Signature
Good Carbs Versus Bad Carbs View by IGphotography from Getty Images Signature

Something surprising is happening in the U.S...


Being fit and balanced doesn’t mean extreme. It’s...

There’s a lot of noise out there about GLP-1 meds...

Starting a fitness routine or healthy eating plan...



Losing weight is a major accomplishment. But even...
